I find this very hard to interpret. A longitudinal ordinal model (e.g. this can let death override all other categories and provides a clinically interpretable treatment effect.
2 Likes
Thanks Andrew,
I agree, however it would probably be less subject to challenge if the expired patients were only assigned the worst possible mSOFA score, rather than a higher score that is not on the mSOFA scale.
Interestingly, the protocol for the study did not specify omitting patients who died prior to the 96 hour mSOFA primary endpoint. While some extremists would likely reject the idea of retrospectively re-including those patients in the analysis using either the worst possible mSOFA score or their latest mSOFA score prior to death, it would be interesting to see such analyses to see what effect survivorship bias had.
I agree with your final takeaway that
While I tend towards the “extreme” that
albeit not just based on the CITRIS-ALI evidence, I recognise that many do not share that view and further trials are necessary for IV vitamin C (IVC) treatment to be widely accepted. I do however believe that the low cost, proven lack of harm and likely benefit of IVC warrant intensivists who are not involved in such further trials giving serious thought to at least trying IVC while they await further results. Especially with the tragic increase in sepsis due to COVID-19, intensivists will likely quickly notice whether or not IVC reduces mortality as much as CITRIS-ALI suggests. Even if a perceived benefit were to turn out to be a placebo effect it would still represent a significant number of lives saved.
Even if IVC treatment became so widely accepted in ICUs as to make IVC vs placebo RCTs impractical, there would still be ways of testing IVC treatment. For example:
-
The apparent success of IVC in CITRIS-ALI implies that earlier implementation could be expected to reduce the number of patients developing sepsis and requiring transfer to the ICU. The success or failure of such early IVC intervention in RCTs would significantly strengthen or weaken the case for using IVC for sepsis.
-
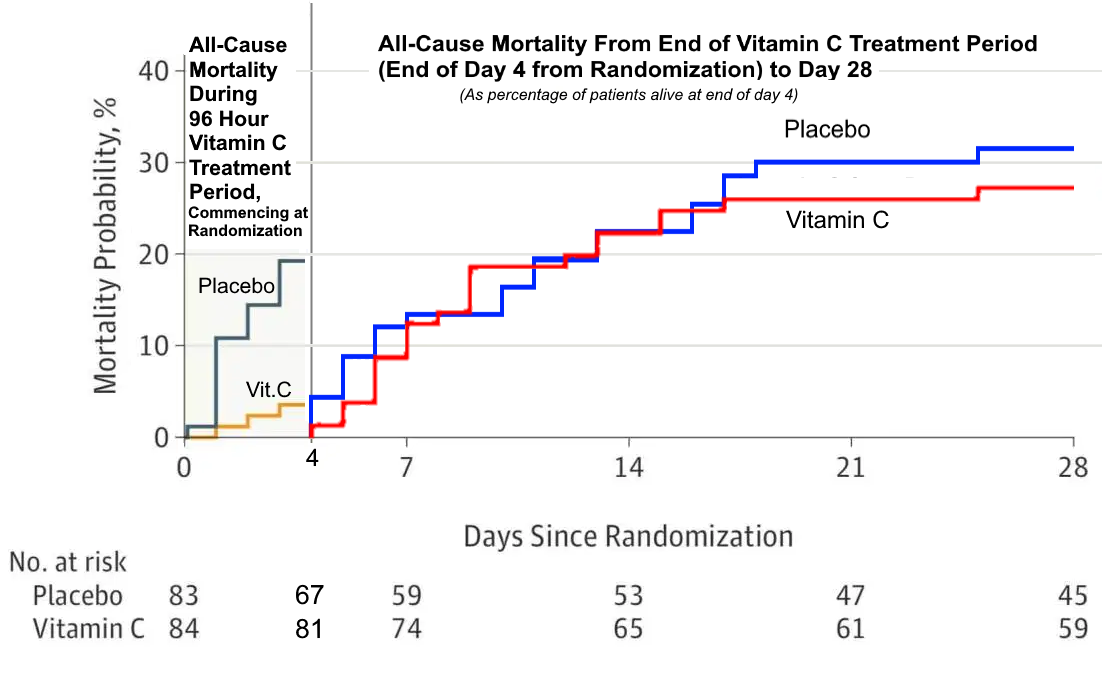
Adjusting the all-cause mortality chart (figure 3.) to compare mortality from Day 5 onwards (See image below) shows substantial similarity between placebo and IVC, which suggests to me that a longer course of IVC may have been beneficial. RCTs examining this hypothesis could still be done without denying patients IVC in the first 96 hours. While a negative result would not significantly change the status quo, a positive result here in a sufficiently powered study would strongly reinforce the evidence for IVC. Such a trial should ideally taper off vitamin C supplementation at the end of treatment so as to avoid withdrawal scurvy.
1 Like