Yes. The Petty/Bone RCT is a term used for a unique pathological modification of the RCT which dominates critical care science. Two USA pulmonologists, Thomas Petty (1960s) and Roger Bone (1980s) developed the idea. The PB RCT applies a research shortcut which allows easy case finding and the use of a single RCT to test a treatment on a variable mix of different (but similar appearing) diseases called “heterogenous syndromes” (ARDS, Sepsis, AKI).
This PB RCT shortcut has been the standard research technique in the US critical care science for ~35 years. The PB RCT was exported decades ago and all countries were intellectually colonized to believe this is a valid derivative of the RCT.
In a PB RCT case finding is rendered easy by the use of threshold sets which are used to quickly triage the cases for inclusion. This is very easy as there is no target disease to diagnose whatsoever. The triage technique for inclusion in a PB RCT deploys a set of non-disease specific consensus set of thresholds which are generally best guessed by a consensus group (called a “task force”) and amended (re-guessed) by a consensus group every decade. This is the standard method of research in critical care. This would be an interesting social “cargo cult” it it were not so dangerous for the public.
In a sense this goes beyond pathological science. It is a form of assembly line case finding for “research” with the trappings of Fisher and Hill strapped on later. So the PB RCT is an RCT façade. The PB RCT is a self-perpetuating form of pathological science as described by Langmuir. Therefore, as with all pathological sciences, of course PB RCT are mostly negative but the few that are positive are not reproducible. This unrecognized pathological science has been the standardized “RCT” technique in critical care science with each new generation being taught the technique.
Statisticians were not told that the heterogenous syndrome under test was connected only by triage and only by case finding set of thresholds, and not by any common biological driver target. So statisticians thought they were doing Fisher/Hill RCT and that the “heterogenous syndrome” was a disease equivalent. In a sense the PB RCT is a pseudo-RCT of synthetic syndromes that are 1960-80s social constructs. An idea of a simpler time when we all thought similar appearing diseases must have a common driver. Now its too late to expose without breaching the veil of political expediency. As we all know, but are not allowed to say, “The spice must flow” (Dune 1)
No one will discuss the PB RCT because virtually all of the critical care research is based on these synthetic syndromes and PB RCT methodology. In the US the PB RCT is not subject to deep introspection so no one debates the validity of PB RCT, even on this forum.
You will never see an advocate of PB RCT openly discuss the method anywhere. For those who understand its presence it is a USA critical care science secret. The rest of the indoctrinated have no idea. Yet, after witnessing 35 years of failure we are trying to shine light on this pathological science. We know this is almost impossible to believe.
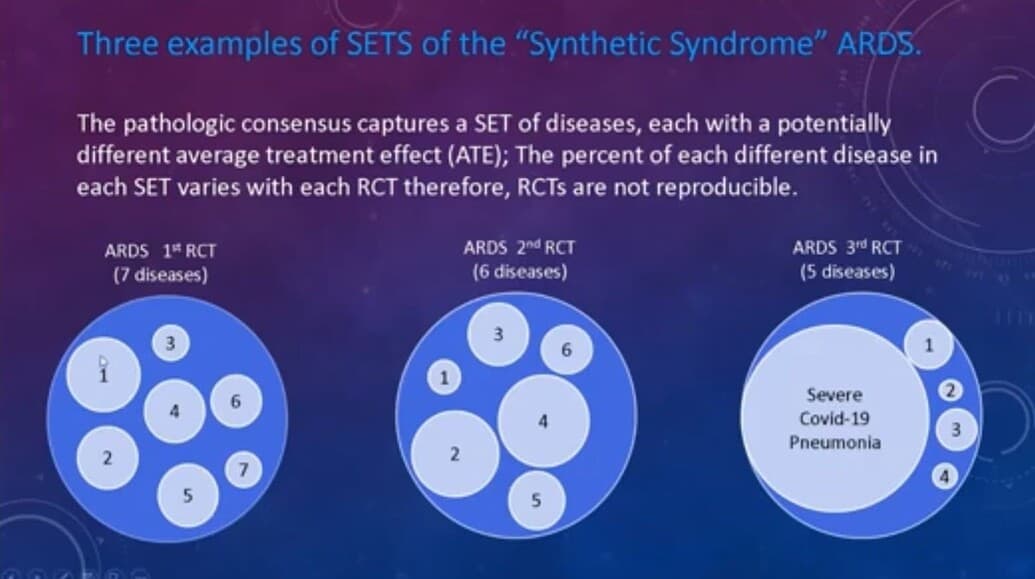
Yes dichotomization is a common pitfall and the Petty/Bone RCT has that problem but the pathology of the PB RCT is much deeper than that. PB RCT are RCT applied to a variable set of different diseases which are lumped together by pathological consensus. The diseases have different drivers. The mix of diseases changes with each new RCT so the the entire set is a moving target. So dichotomization, as a function of the entry criteria, is only a small part of the problem.
In the most dramatic example, a specific standardized Ventilator treatment was tested by PB RCT on ARDS (as a lumped set) and found to reduce mortality so this was applied, as evidenced based, to COVID pneumonia (which met the standard PB RCT criteria for ARDS). This treatment failed causing much loss. This shows that the unwillingness to deeply and publicly debate critical care research methodology and openly introspect, has real adverse consequences for the public health at the bedside.
So, the pathology of the PB RCT is magnified by the dichotomization problem but beyond that the PB RCT is a unique type of pathological science which is not subject to analysis as a function of expediency.
Yes. Excellent. Also R varies with the mix of different disease captured by the consensus threshold criteria with each new PB RCT. So mathematically, reproducibility should not be expected.
This is not a Fisher/Hill RCT. Its really not an RCT in the sense that Hill described it so no one should wonder why they all fail. Its not based on a valid function, so it is not real science
Despite this, the validity of the PB RCT is the one subject which no one will discuss (except in this forum) which is why almost no one knows about the PB RCT. Everyone inside critical care science knows that that the state of critical care research is in severe crisis but the idea that the fundamental methodology, in which all (including myself, in the 1980s) were indoctrinated, might be pathological is simply too much for the experts to bear so the PB RCT are simply funded and performed and are not subject to scientific self correction.
We have many allies and are hoping ex-US scientists and statisticians will lead the USA out of this harmful abyss. We call ourselves the critical care rebels. We seek open debate to let the young decide for themselves.
We blame no one. We were all indoctrinated and who is not guilty of failing to timely pull up a well barnacled anchor. Yet we don’t want the youth to be indoctrinated as we were. Exposure to open and candid antidogmatic debate is their right as scientists. No one has the right to capture their minds, even unknowingly. Reform will follow when debate is allowed. Yet the debate gate is closed, the young brilliant horses are trapped in the “dogma stall”.
As a test, try to convince one or more of your brightest, most pugnacious, and debate favoring critical care expert scientist here to debate on this thread now. They will decline. Silence is the only defense they have.