What is the value of presenting patient-specific treatment effects in RCT/IPD-MAs articles?
Background
In this individual patient data network meta-analysis (IPD-NMA), the authors presented patient-specific treatment effects, along with a nice Shiny app.
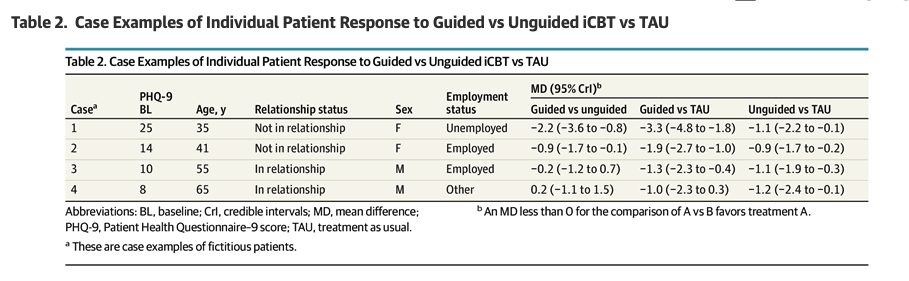
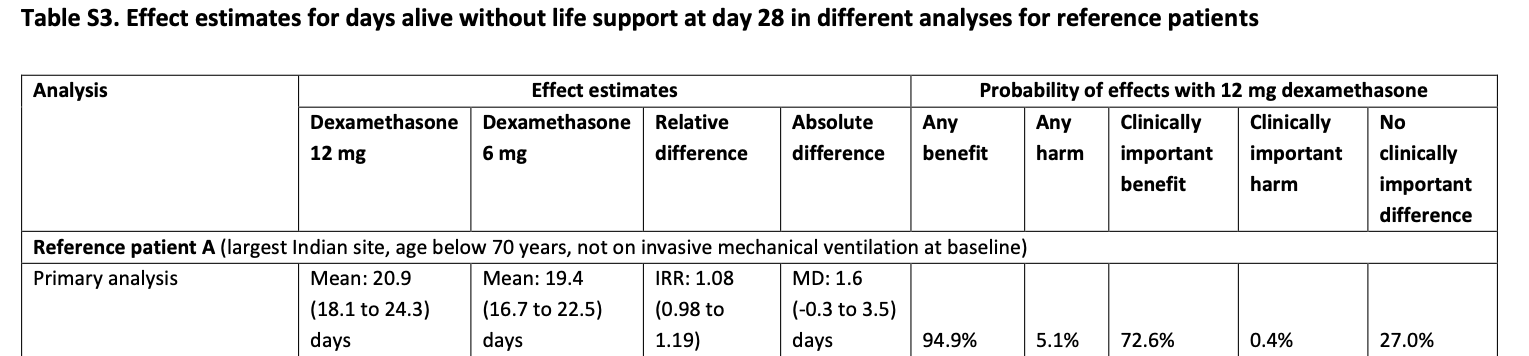
Similarly, in this randomized clinical trial, @granholm et al. calculated estimates for three different representative reference patients, e.g.:
Dr. @f2harrell has suggested that picking reference patients to present absolute risk differences (in logistic regressions) is a suitable approach:
Prognostic
There was no clear goal of developing a prognostic score in both examples above.
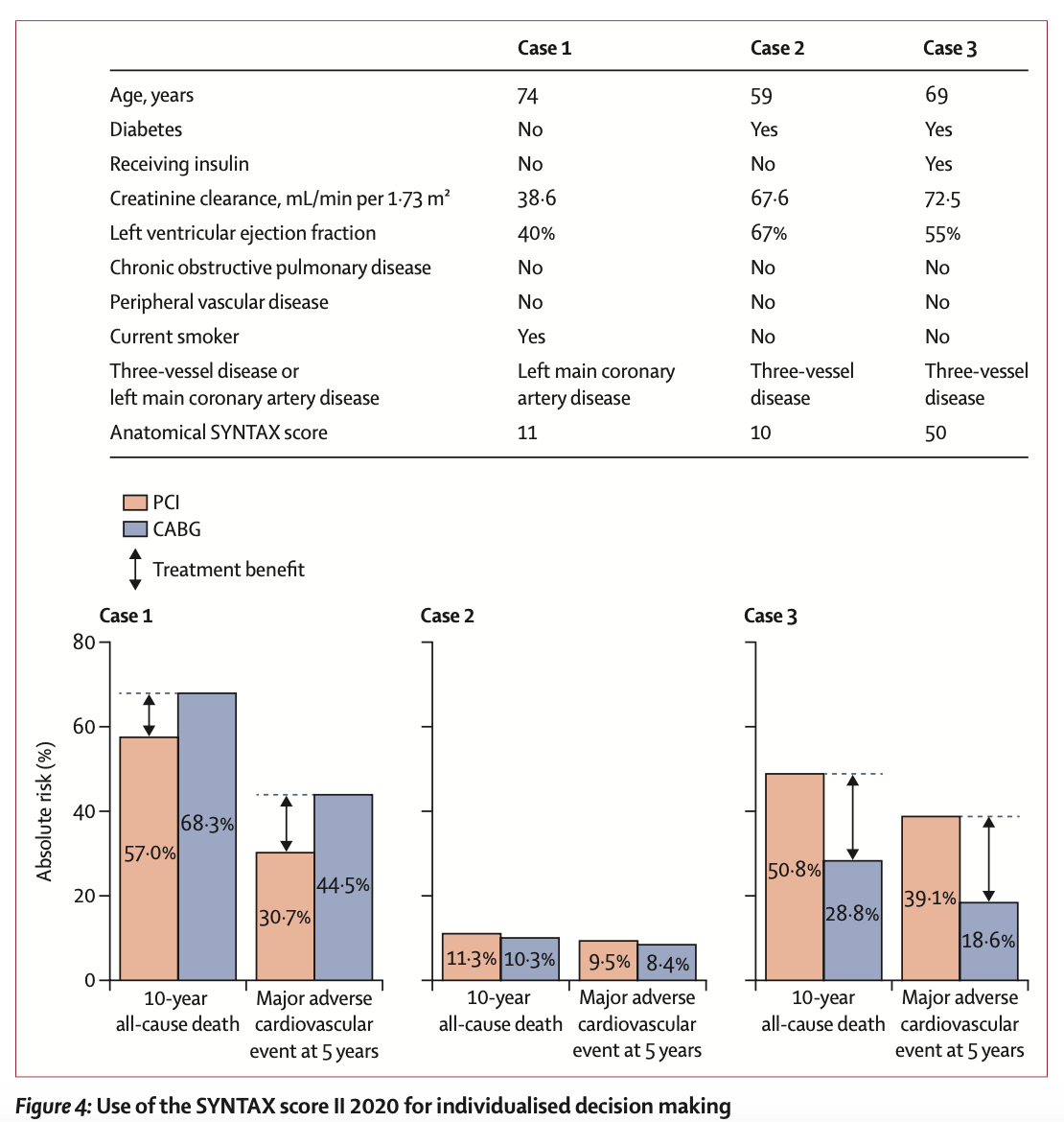
On the other hand, in this other study, @Ewout_Steyerberg and colleagues developed a prognostic score from one RCT, and validated it externally using IPD from three other RCTs.
They then present this figure to depict the application of such score in three different representative reference patients:
Question
When there is no predictive goal, what are the advantages of presenting patient-specific treatment effects along with conditional/marginal relative effects in RCTs/IPD-MAs?