As an antidote to the overweening inductivism of EBM, I have previously advocated that we direct more attention to the theories underlying medical therapies, and devote more effort to their critical examination. Stimulated by the recent social-media kerfuffle over thrombolysis in acute ischemic stroke, I licensed the NINDS data with the intent to pursue a model-based examination of the penumbra theory that underlies this therapy.
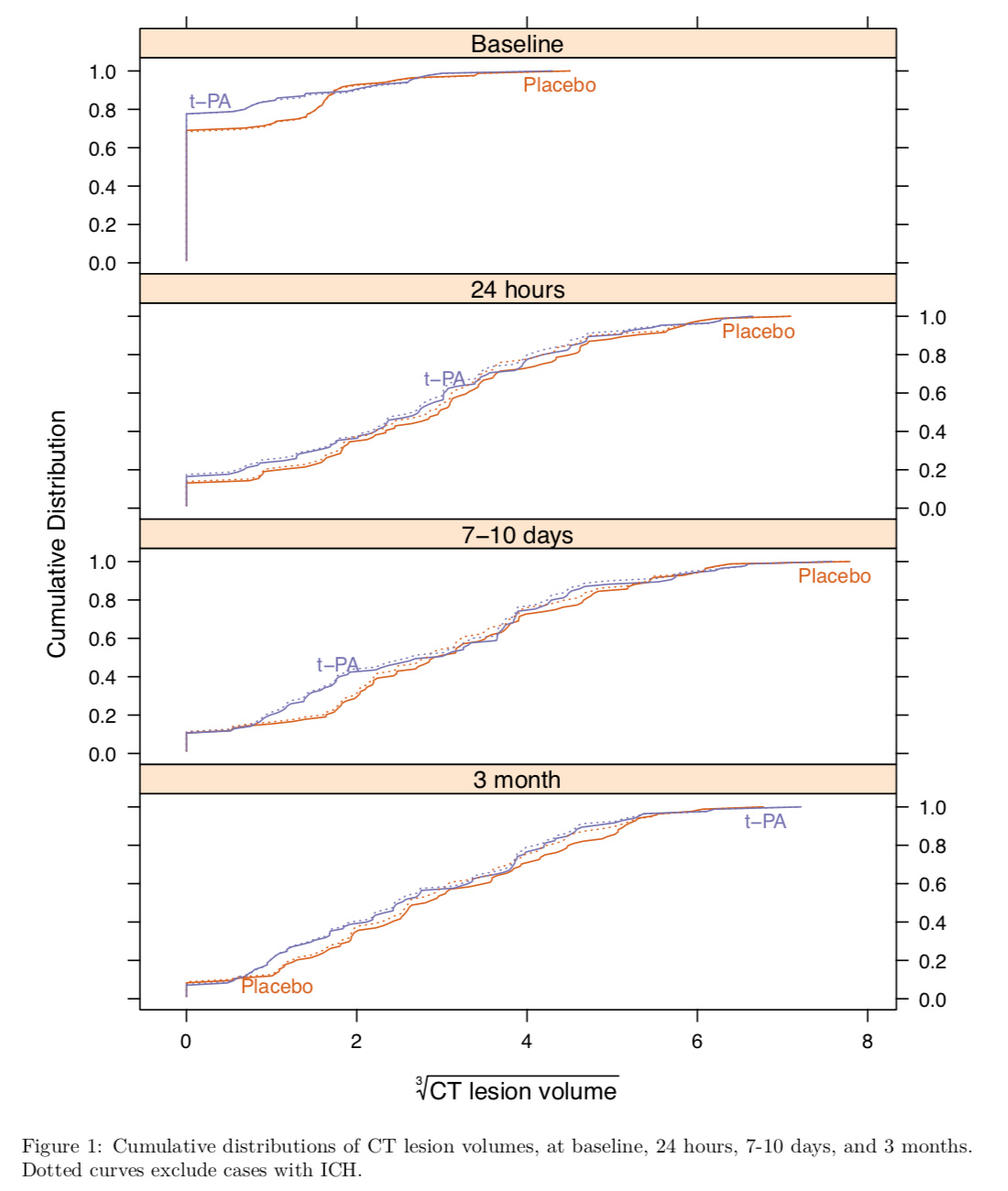
In my initial graphical exploration, however, I’ve uncovered rather less evidence than I’d expected for an impact of thrombolysis on infarct volumes by CT imaging. Here’s the full exploration at my public GitHub repo, where you’ll also find code for the analysis and data preparation. (I cannot distribute the data, unfortunately, but perhaps I could get a collaborator added to my license reasonably quickly.) The short story is basically that empirical cumulative distributions of infarct volumes look like this, even after restricting attention to the most common single type of stroke (cardioembolic):
This greatly dampens my enthusiasm for investing effort in formal modeling, but I’m acutely aware that I lack detailed knowledge of stroke imaging that may be necessary for the efficient extraction of information from the infarct volume measures in NINDS. Would anyone be aware of prior attempts to examine the penumbra theory in this manner? Would anyone with more domain expertise care to collaborate with me on this analysis?
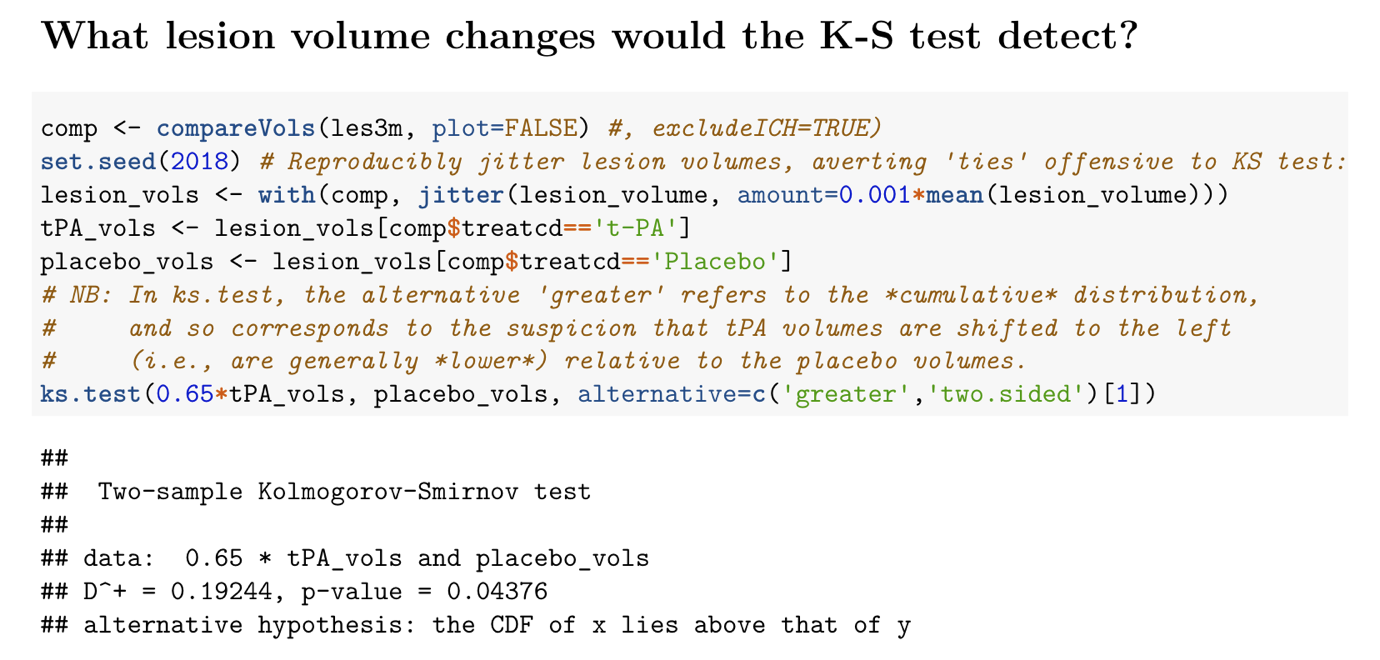
Just by way of quick follow-up… I’ve since added the further analysis below, in which I enquire what effect size would have been required to yield a ‘significant’ Kolmogorov-Smirnov test. The answer (0.65 => 35% infarct volume reduction) underscores my earlier impression that more ‘shoe leather’ (or, since collaboration with a radiologist is required, ‘butt-leather’) will be necessary to deliver any useful interrogation of the penumbra theory using NINDS data.
David, I am struck by your comments
“I’ve uncovered rather less evidence than I’d expected for an impact of thrombolysis on infarct volumes by CT imaging.”
If lytic therapy improves outcomes - should it not follow there should be an effect on CT scans.
John, the modus tollens argument you put forward would be precisely my (Popperian/falsificationist) point. More broadly (say, from the POV of Popper’s more fully elaborated critical rationalism), we know our knowledge is always faulty and that the obligation to critically test it never ends. The best way to “keep on keepin’ on” in criticizing our knowledge about medical therapies is to criticise the theories that constitute the deepest part of this knowledge.
If the penumbra theory were true, one would expect to be able to find a signal to this effect in CT infarct volume time-series. One valuable aspect of these time-series data (relative to mRS-type outcomes) is that they are quantitative and possibly more objective in terms of inter-rater reliability.
Are you aware of any existing analysis in the literature, that attempts to check the penumbra hypothesis? I must suppose that natural variation present in observational clot aspiration registries would provide an excellent basis for demonstrating penumbra evolution to infarct—with onset-to-aspiration time providing the instrumental variable. (Disclosure: I was at AAN 2015, where I ‘got religion’ on that account.) Conceptually, that’s the type of thing I had hoped to find possible in NINDS.
For context, and to make explicit the “social-media kerfuffle” mentioned above, I’ll link one of the more ambitious summaries on the topic https://first10em.com/thrombolytics-for-stoke/. It’s from the EM crowd, and I think their read on the evidence is important because they’re often the ones pulling the trigger on this treatment. It should in no way be seen as a discouragement of your line of investigation @davidcnorrismd, but to me it seems like it might be looking at a proposed mechanism of an effect that does not exist (or only exists in very select patient populations). Eager to see what you can make of the NINDS data!
Many thanks, Martin! Just to be clear, I greatly appreciated the service @drjohnm performed in bringing this “kerfuffle” to wider attention with his Medscape article. I had also seen some of the First10EM tweets/posts during that time-frame in the Spring, but not the comprehensive review you linked. Upon a cursory scan of this, I find only ATLANTIS A included infarct size as an outcome, and I see nothing mentioned in the way of a ‘finding’ in that regard.
I am entirely open to the possibility you raise, that IV tPA may not actually be rescuing the penumbra systematically in AIS. Whereas I embarked on this analysis mainly in the hope it would allow me to pursue a methodological agenda (for transparency, I’ve just pushed my original Data Request Form, which includes my Scientific Purpose statement on p. 2), I do now think the present state of my data exploration presents a problem for the pro-tPA camp. I would hope someone from that camp with a sincere belief in IV tPA in AIS might take up the challenge of collaborating with me.