Dear Colleagues. I want to share with you my most recent paper published. I would like to open the discussion about Joint Model analysis applied to RCTs. Sincerely, Oscar Leonel Rueda-Ochoa. Erasmus University Medical Center.
Questions to start the discussion
Do you have previous experience doing Joint model analysis under RCTs? Could you give us some examples of its applicability?
Could Joint model analysis be applied to all RCTs? What do you think is the best scenario for applying it under RCTs?
What do you think are the advantages and disadvantages of this statistical analysis?
What is your opinion about Cumulative Joint model analysis applied in SPRINT trial (paper attached)
some have used a ‘global rank composite’ as the primary outcome of an RCT, combining survival outcomes and a biomarker. I’m not sure if anyone has done it, but i think it would be worthwhile comparing the performance of a global rank and a joint model … actually, i think someone did it in ALS
Dear Paul, thanks for your comments and for the paper shared. Your question about to adjust for a post-baseline covariate is so interesting. One of the problems to do this is the possibility to produce bias results if this covariate is a mediator of the relationship among the intervention (treatment) and the outcome. Adjusting for a time varying mediator covariate produces the effect of treatment waned down with time. Advantages of Joint model is that you could evaluate post-baseline time-varying covariates (i.e SBP) as and outcome and not as a covariate. In addition, the random part of the linear mixed model could include others time varying covariates (i.e SAEs) as latent variables. Let me give to you an example with my paper:
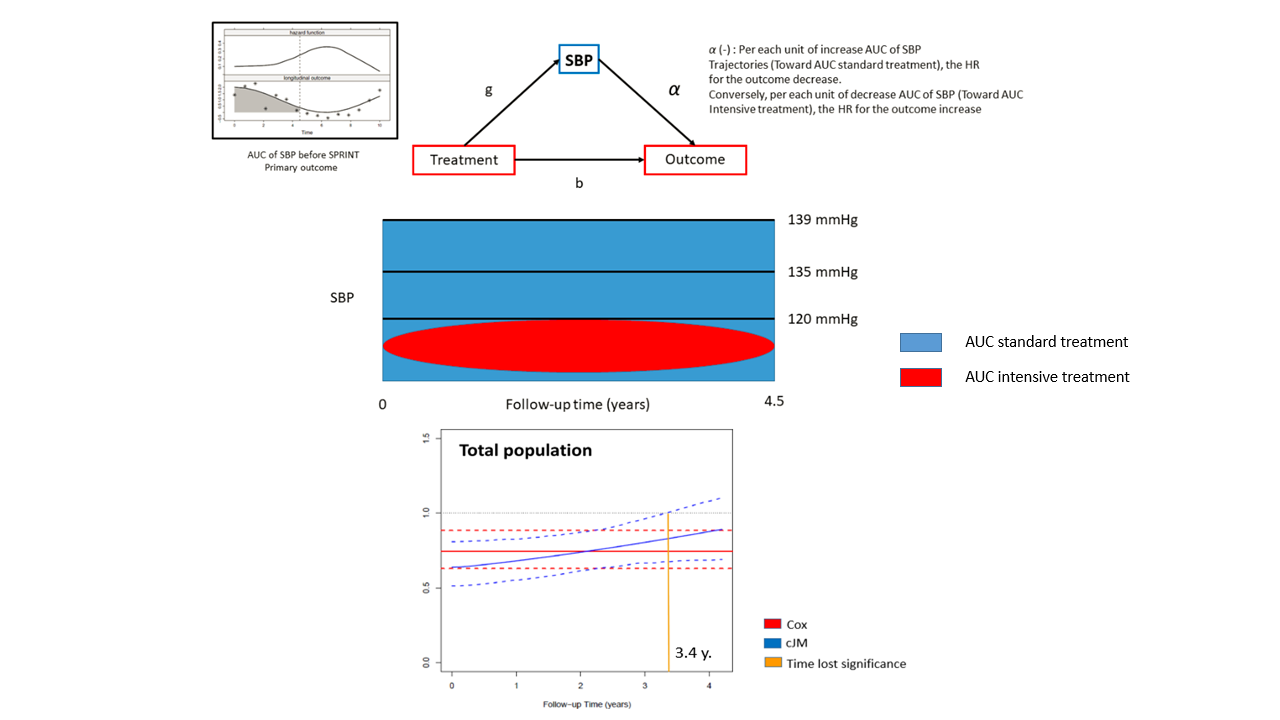
Our interest was to evaluate if the efficacy of systolic blood pressure (SBP) intensive treatment over SPRINT primary outcome could be affected by cumulative SBP, SBP intra-individual variability and serious adverse events (SAEs) produced during follow-up. In our case, we build a cumulative joint model that include a linear mixed model (LMM) + a traditional Cox proportional hazard model. In the LMM the outcome was SBP repeated measurements over time, adjusted by time, treatment and interaction among time:treatment. No others covariates because both groups were balanced by randomized at baseline. The fixed part of this model include SBP variability between interventions groups and the random part of this model include intra-individual SBP variability and other time varying covariates as latent variables (i.e SAEs). Please see graph below.
In the case that we want to evaluate the impact that SAEs has over SPRINT primary outcome, we used other approach: We created an interaction term between SAEs: treatment into cJM. This interaction was statistical significant (p<0.0001), so we decided do a stratify analysis comparing two groups: people with and without SAEs under cJM. Please see graph below
We found that SBP intensive treatment reduce its beneficial effect in people who suffer SAEs than people without SAEs (HR is less protective 3 times). In addition, this beneficial effect is loss early in participants with SAEs (loss effect at 3.4 years) compared with participants w/o SAEs (4.2 years).
Dear Colleagues. I want to share an editorial comment to my paper published in print version in the issue of May 2019 in Journal of hypertension. Sincerely, Oscar Leonel Rueda-Ochoa. Department of Epidemiology. Erasmus University Medical Center.
Very interesting re-analysis of SPRINT. It would be interesting to supplement that with an analysis that incorporates clinical severity of various outcomes, or that uses patient utilities for these. For example, a repeated ordinal analysis of SBP with SBP overridden by various clinical events would be interesting. As I understand your reanalysis, no judgment was made regarding whether a large lowering of SBP in a patient could partially offset a clinical event in another patient.
Dear Professor Harrell, thank you very much for your comments. Our cumulative Joint model analysis did allow us to evaluate the impact that lower cumulative SBP has on the Hazard ratio of the primary SPRINT outcome. We found that a large lowering of SBP (<120 mmhg) sustained in time (lower AUC), produced by intensive treatment compared with standard treatment, increases the hazard ratio of the primary outcome. Consequently, the initial protective effect of the intervention is gradually lost until no significance after a 3.4 year follow-up in the total population. (Follow-up range from 0 to 4.5 years).
This same phenomenon is observed not only in the total population, but especially in some subgroups such as women, black participants, participants with previous history of CV disease or CKD and, younger 75 year. Unfortunately, the limited number of outcomes limits the power for a specific outcome analysis and only allows us to analyze the composite outcome.
All the commands, step by step, used in our analysis and the outputs of our model, can be consulted for their replication in the following link of the supplementary material.
Very nice. What I’m getting at that would supplement that is an analysis of overall graded outcome where they are graded such that there is a reward for lower SBP and a penalty for clinical events, with no binning of SBP. An overall ordinal outcome variable is one way to do that.